2021-06-15 update: Medical researchers agree that there is no reason to vaccinate kids against COVID-19, but they are frightened to go against the faux consensus, and have to word their opinion cautiously.
Vaccinating children against SARS-CoV-2. Hard to justify right now for most children in most countries.
Young people have been largely spared from severe covid-19 so far, and the value of childhood vaccination against respiratory viruses in general remains an open question for three reasons: the limited benefits of protection in age groups that experience only mild disease; the limited effects on transmission because of the range of antigenic types and waning vaccine induced immunity; and the possibility of unintended consequences related to differences in vaccine induced and infection induced immunity.
Lavine J S, Bjornstad O, Antia R. Vaccinating children against SARS-CoV-2. BMJ, May 13 2021
2021-05-10 update: FDA has purportedly authorized Pfizer COVID-19 vaccine for emergency use on children 12 – 15 (the letter & press release). This reckless authorizations is signed by the same Denise Hinton, who wrote crooked restrictions into the EUA for HCQ, and then withdrew that EUA. Giving children 12-15 this vaccine would be a crime, regardless of consent of the victim. end of the update
It is very painful to watch young people (original meaning was ages 18-30) forced and/or tricked into getting COVID-19 vaccines they do not need, just because it is the policy. Those under the age of 45, without well-known preexisting conditions (obesity, diabetes, hypertension, & few more), are almost at zero risk of dying from COVID-19, and they have a very low chance of experiencing any serious form of the disease. For these young people, the short-term symptoms of a COVID-19 vaccine are more serious than what they would experience from the disease itself. Besides, most of these young people already have at least some immunity from natural exposure to the Wuhan coronavirus. One can develop immunity to COVID-19 without experiencing any symptoms.
The most used in the US COVID-19 vaccines are from Pfizer and Moderna. They are mRNA vaccines. These are the first mRNA vaccines that have ever been approved, and they were approved for the emergency use only. mRNA vaccines are a great scientific breakthrough, on the same level as the discovery of antibiotics. However, the downside is that their long-term effects are still unknown. mRNA vaccines are different from anything that exists in nature. Not a single person in the world received an mRNA vaccine for COVID-19 and was observed for even 15 months. Maximum a few dozen individuals received any other experimental mRNA vaccine and were observed for a few years. AstraZeneca and J&J vaccines are viral vector vaccines. It is also a relatively novel vaccine type.
These brand new COVID-19 vaccines should not be given out like candy. For most people under the age of 45, they provide zero benefit and unknown long-term risks. It is irrational for these young people to take such a vaccine. Even worse, the authorities have started vaccinating children. 2.3% of the children received at least one dose of COVID-19 vaccine (See CDC breakdown by age on April 25, or the current one). All this while 20% of people over 65 have not even received one dose. People 65+ do need vaccination against COVID-19. The most logical course of action would be to focus on vaccinating the 65+ population. Vaccine doses should be reserved for them, for those with conditions increasing risk. After some additional reserve is maintained, the excess doses can be given to countries that need them for their at-risk population.
Natural Immunity Acquisition
There has been a continuing decrease in life threatening COVID-19 infections since their peak during the 2020 Christmas – New Year holidays. The decrease is in the 25-44 age bracket is noticeable. It can be seen on the mortality chart, considering that deaths trail infections by an average of 4 weeks.
Deaths decreased 4x, from 525 on the week ending 1/23 to 134 on week ending 3/13. This data corresponds to infection data from the week ending on 12/28/2020 to the week ending on 02/13/2021. Vaccinations were not a factor in this age bracket. Season remained the same. Treatment did not improve during this time period. The only factor was natural immunity acquisition.
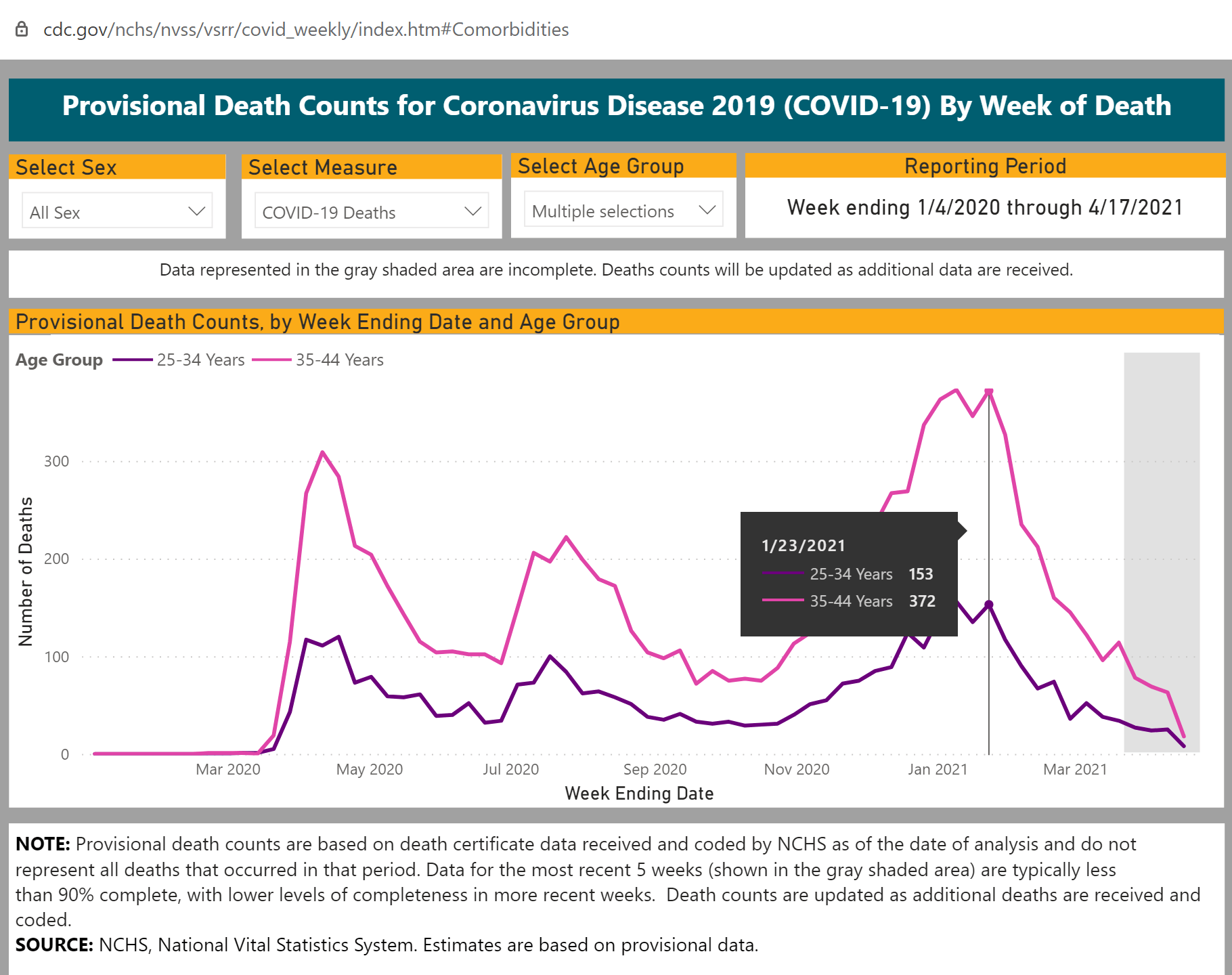
https://www.cdc.gov/nchs/nvss/vsrr/covid_weekly/index.htm#Comorbidities
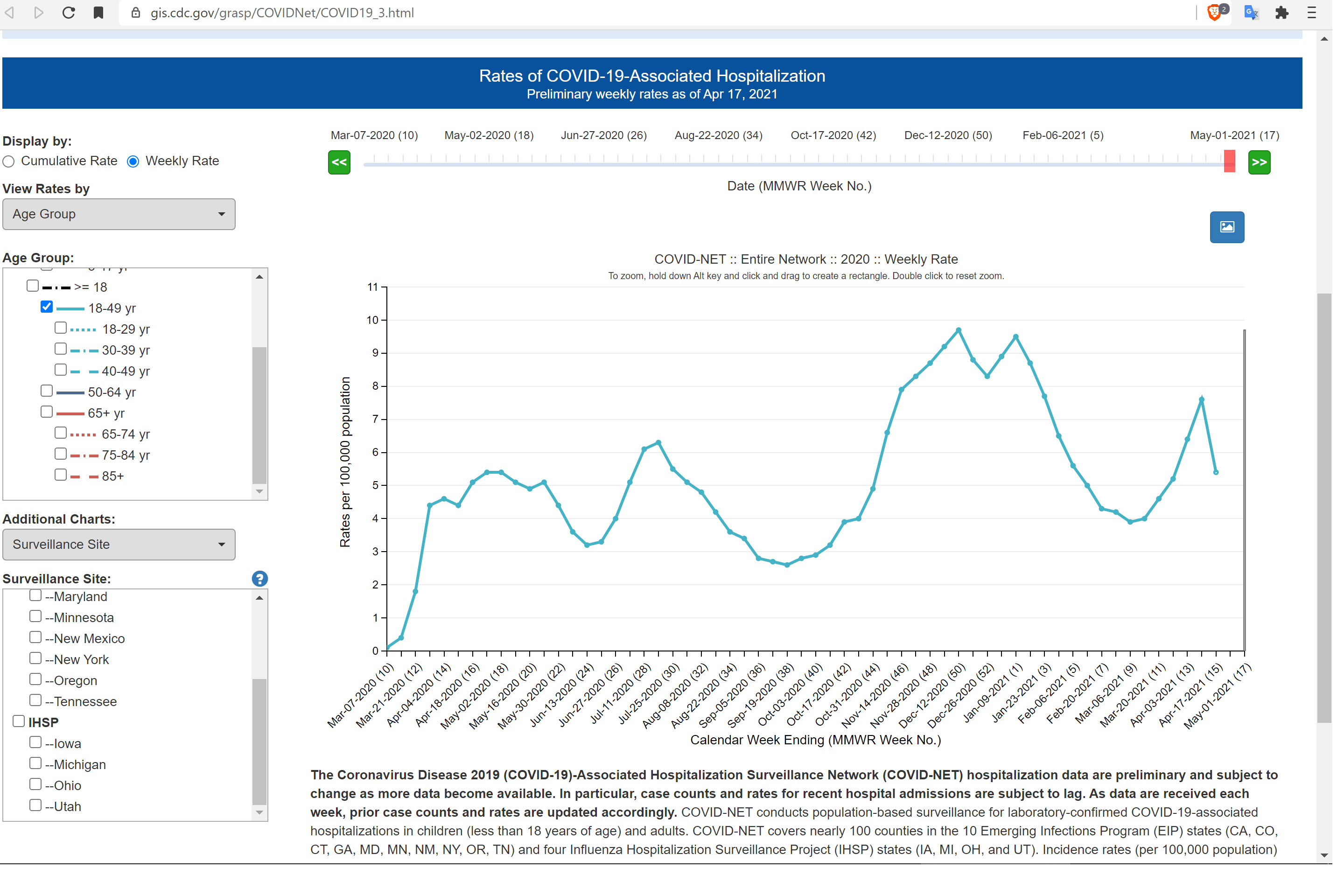
This dynamic is confirmed by hospitalization data. There has been a steep decline in COVID-19 hospitalizations for the matching period, the week ending 01/09 to the week ending 02/27. There is an average two week lag from a serious infection to a hospitalization.
https://gis.cdc.gov/grasp/COVIDNet/COVID19_3.html Ages 18-49. The data is for a subset of states, including California and New York but excluding Texas and Florida. Notice the ominous peak on the week of April 10.
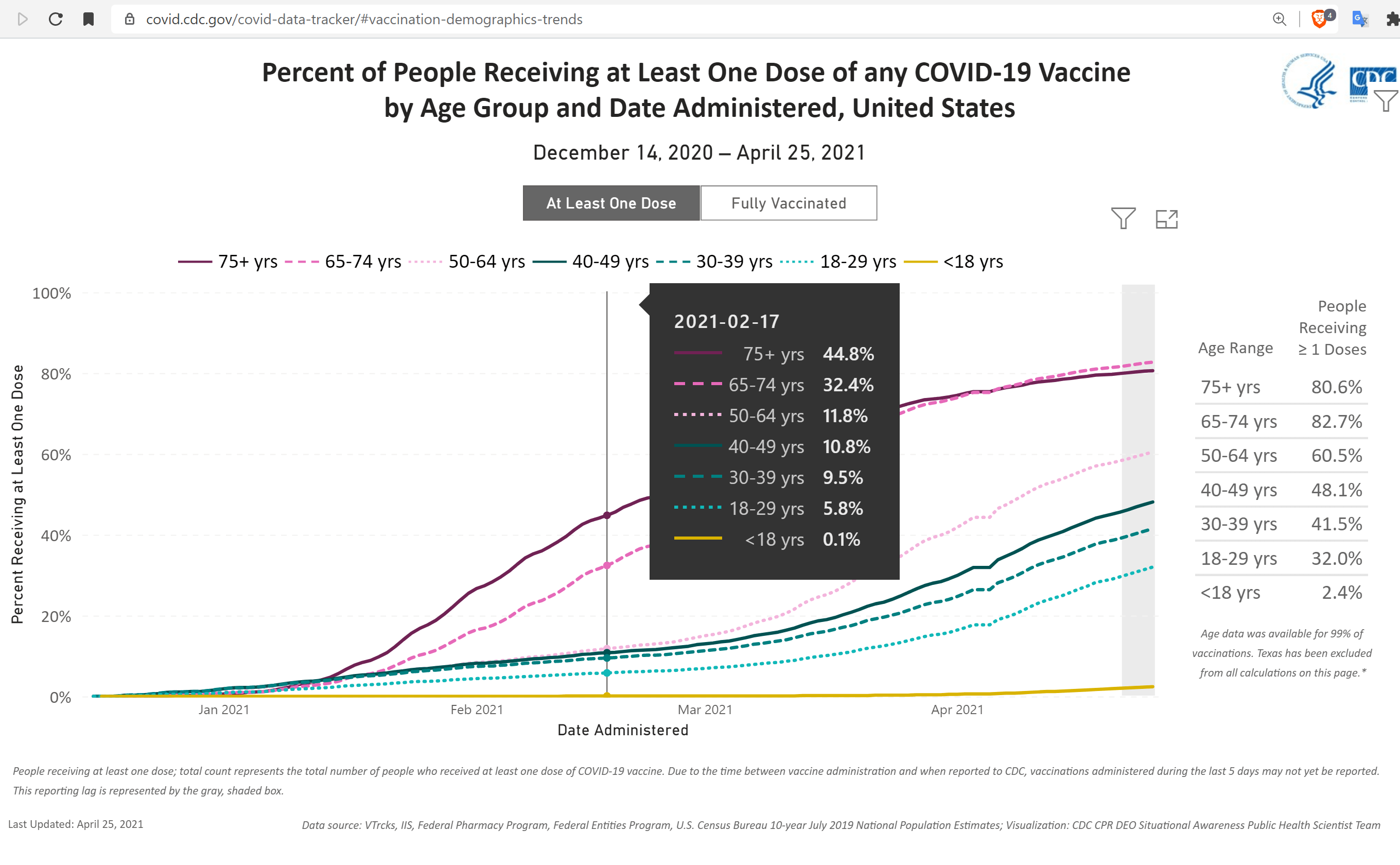
The following chart shows that vaccinations were not a factor in the decrease in mortality in the 25-44 bracket. Only about 10% of this bracket received a vaccine, and those who were more likely to already have immunity were also more likely to receive a vaccine (like health care workers).
 https://covid.cdc.gov/covid-data-tracker/#vaccination-demographics-trends
https://covid.cdc.gov/covid-data-tracker/#vaccination-demographics-trends
Low Risk of dying from COVID-19 under 45
Since the beginning of the pandemic, about 13,000 individuals in the age bracket of 25 to 44 died with COVID-19. About 40% of them had obesity, diabetes, and/or hypertension listed as a comorbidity (it is hard to obtain exact percentages due to the high correlation between these conditions). Obesity is not normally listed as a condition contributing to death, so it is likely that many of the people who died with COVID-19 had obesity, but it was not. Some other conditions increasing susceptibility to COVID-19 were not recorded at all. Chronic conditions, known to increase risk and/or severity of COVID-19 are likely underreported. Thus, the number of healthy non-obese people 25-44 years of age, who died from COVID-19 over the pandemic is somewhere between a few hundreds and 8,000. Even those who died did not have to die, because effective treatments have been available since early last year.
Compare this number of COVID-19 deaths to more than 30,000 annual drug overdose deaths in the same bracket. Or compare it to approximately 12,000 annual motor vehicle deaths in this age bracket, at least half of which are not at fault (25-34, 35-44). And yet, no one is suggesting that we stop driving. For a healthy non-obese person below age 45 the chances of dying from COVID-19 were less than the chances of dying from an auto accident. The risk is even lower now when most of these people have acquired some immunity. They do not need vaccination.
Remarks
Technically, mRNA vaccines did not even fall under the dictionary definition of a vaccine (Cambridge Dictionary), until online dictionaries started changing the definition in 2021, like Miriam-Webster did.
The chances of dying from COVID-19, below the age of 25, are too small to even consider here.
WISQARS is a useful statistics tool.
Originally published on April 26.